Treatment Of Pancreatic Neuroendocrine Tumors
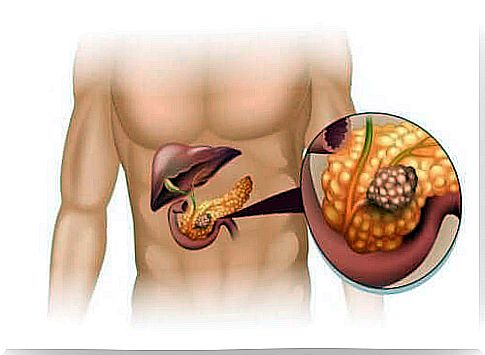
Treatment of neoplastic tumors always depends on their type. Pancreatic neuroendocrine tumors are a group of endocrine tumors that originate from islet cells in the pancreas. Overall, they are not very aggressive, although they can be potentially malicious. In this article, we describe the types and treatments of pancreatic neuroendocrine tumors. Please read carefully!
Types of pancreatic neuronendocrine tumors
Tumors produced in the islets of the pancreas can be of two types: functional and non-functional.
Functional tumors
When tumors belong to the functional group, there is an excessive secretion of hormones. These types of neoplasms mainly include:
- Gastrinoma: is a tumor that secretes gastrin. Responsible for the hypergastrinemia of the Zollinger-Ellison syndrome.
- Insulinoma: This is one of the most common pancreatic neuroendocrine tumors. This is a pathology in which insulin is produced in excess. However, it is usually mild in nature.
- Glucagonoma: This is a malignant tumor. There is an increase in the concentration of glucagon secreted by alpha cells in the islets of the pancreas.
- Somatostatinoma: This is an extremely rare and usually malignant tumor. This tumor also contributes to the excessive secretion of somatostatin.
- VIPoma: This type of cancer has a low incidence and also affects the hypersecretion of the intestinal polypeptide.
- ACTHoma: ACTH is an adrenocorticotropic hormone. When islets over-secrete this hormone, rapidly growing tumors emerge.
Non-functional tumors
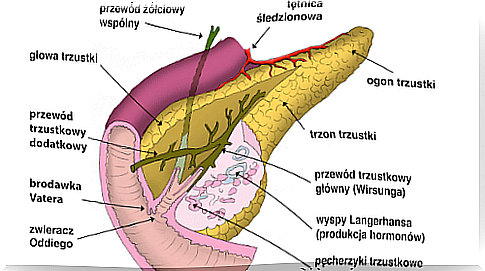
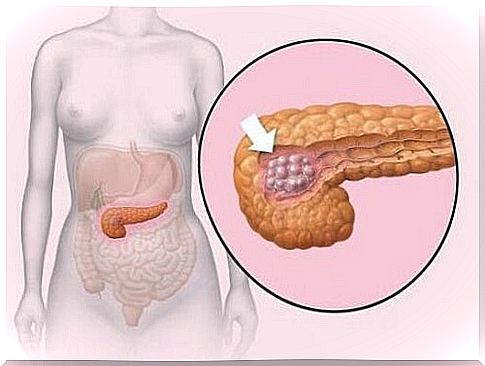
About half of these tumors are found in the head and neck of the pancreas. Among non-functional tumors, PPoma is the most common. These tumors do grow slowly. They are only detected when they reach large sizes and have metastasized. Overall, patients experience symptoms such as:
- Weight loss
- Abdominal pain
- Tangible mass
- Jaundice
Diagnosing neuroendocrine tumors
Diagnosis of pancreatic neuroendocrine tumors requires clinical examination, endocrine tests, imaging and histopathological analysis of the tumor.
Other techniques, such as endoscopic ultrasound and gamma ray somatostatin receptors, also allow you to see metastasis to the liver, lymph nodes, and bones. Immunohistochemistry is also used to determine the degree of tumor development.
Treatment of neuroendocrine tumors
Treatment of pancreatic neuroendocrine tumors largely depends on whether they can be completely removed. However, there are other factors, such as your overall health, to consider when choosing a treatment.
However, it can sometimes be difficult to determine if the tumor can be completely removed. For this reason, having a laparoscopy before surgery will help confirm whether the tumor is removable.
Treatment of resectable tumors
However, most pancreatic neuroendocrine tumors that have not spread to distant parts of the body are resectable. Even some pancreatic neuroendocrine tumors that have spread can be resectable if they have not spread too far.
The operation that is performed will depend on the type of tumor, size and location in the pancreas. Surgery can be simple and just remove the tumor itself, or it can be complex like Whipple’s surgery (pancreatoduodenectomy).
Lymph nodes are also removed frequently. However, after surgery, it is important to monitor your recovery. It is advisable to look out for any symptoms that indicate a relapse or spread of cancer.
Treatment of inoperable neuroendocrine tumors
Unfortunately, these tumors cannot be completely removed surgically. Usually these are slow-growing tumors. In some cases, their development is controlled and medications are prescribed to slow their development.
In patients with inoperable tumors, chemotherapy is usually recommended as the first treatment. As tumors spread beyond the pancreas, patients develop symptoms such as diarrhea and hormonal problems.
The prognosis of neuroendocrine tumors is variable and depends on many factors. The least favorable is that associated with higher grade tumors and the presence of liver and lymph node metastases. The 5-year survival rate in resectable functional tumors exceeds 97%, but is only 30% in non-functional tumors.